


Should subclinical (ctDNA positive) MCC be treated with immunotherapy? A Proposed Randomized Clinical Trial



The MC3 Institute is developing a randomized clinical trial to evaluate whether immune checkpoint inhibition (ICI) should be initiated when circulating tumor DNA (ctDNA) becomes positive, before an MCC recurrence becomes clinically evident. We will determine whether this approach improves patient outcomes, including progression-free survival and MCC-specific survival. We are seeking participation from other centers in this planning phase.
BACKGROUND
Circulating tumor DNA (ctDNA) has emerged as a biomarker for monitoring disease recurrence and assessing treatment response in various cancer types.
Akaike et al. carried out a study of 319 patients with MCC across six US academic centers and 24 investigators [1]. They found that ctDNA has excellent sensitivity of 94%-95% and specificity of 86%-90% for detecting clinically evident disease by physical exams/scans, as demonstrated in two separate groups of patients (test and validation cohorts). These findings highlight ctDNA as a valuable biomarker associated with recurrence risk in MCC. As a result, ctDNA has been included as a recommended biomarker for MCC surveillance in the 2025 National Comprehensive Cancer Network (NCCN) guidelines.
Importantly, the study showed that ctDNA-positive patients with stage I-III (locoregional) MCC, in the absence of visible disease, faced a 7.4-fold higher recurrence risk compared to ctDNA-negative patients (P < 0.001). As such, ctDNA often reveals MCC recurrence months ahead of standard imaging methods.
In the current standard management guidelines, patients who have molecular evidence of disease but not clinically evident disease are closely observed and do not start treatment until their disease becomes clinically evident. There is a need for data regarding whether patients respond better to immunotherapy initiated when there is only molecular evidence of disease (ctDNA positive).
SIGNIFICANCE
A trial would address a key limitation in current adjuvant treatment strategies for MCC. Presently, several adjuvant trials in the U.S., Europe, and Australia are exploring the efficacy of immunotherapy for MCC patients whose risk is higher based on stage alone. If higher stage alone is used to determine who receives adjuvant therapy, 30-70% of patients would be offered immunotherapy, who would in fact never have developed recurrent disease.
ctDNA offers an approach to “de-escalate” adjuvant therapy by offering it only to patients with the highest risk of developing disease. Indeed, >90% of patients with ctDNA positivity and negative scans will go on to develop clinically evident disease within 1-2 years.
If early initiation of immunotherapy for subclinical MCC in ctDNA-positive patients improves disease progression-free survival or MCC-specific survival, it could fundamentally shift current management paradigms.
Because ctDNA is now being adopted for ongoing surveillance, earlier identification of patients with low level disease is becoming routine months or even years after initial treatment.
PROPOSED TRIAL
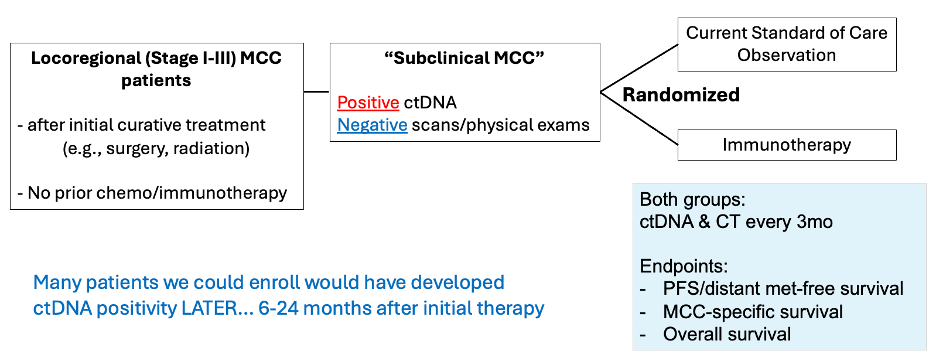
MCC patients who had been treated with surgery/radiation and developed ctDNA positivity at any time could be eligible for the trial if they do not have clinical evidence of disease. Interested patients would be randomized to observation versus initiation of immunotherapy. Both groups would have ctDNA testing and CT scans every 3 months.
Trial subjects would be assessed for the primary end point (disease progression) as well as overall survival, safety, and quality of life. Additionally, the fraction of patients who become ctDNA negative and T cell immune biomarkers will be studied.
COLLABORATE
If you would like to join us in developing this trial, please reach out to: mc3institute@uw.edu.
1. Akaike T, Thakuria M, Silk AW, et al. Circulating Tumor DNA Assay Detects Merkel Cell Carcinoma Recurrence, Disease Progression, and Minimal Residual Disease: Surveillance and Prognostic Implications. J Clin Oncol. 2024 Sep 10;42(26):3151-3161. https://ascopubs.org/doi/10.1200/JCO.23.02054



